

BES2024 BES 2024 CLINICAL STUDIES (17 abstracts)
The value of liquid and solid mixed meal tests to diagnose postprandial reactive hypoglycaemic syndrome (PRHS)
S. Desmedt , J. Marlier , F. Van de Velde , Y. Van Nieuwenhove , I. Matthys & B. Lapauw
Ghent University Hospital
Objectives: Precise diagnostics for postprandial reactive hypoglycaemic syndrome (PRHS) after gastric bypass surgery (GBS) are lacking. Oral glucose tolerance tests (OGTT) are advocated but might cause early dumping and lack specificity. In this observational study glycaemic responses during liquid and solid mixed meal tolerance tests (LMMTT and SMMTT) were evaluated.
Materials and methods: Twenty-two subjects at least one year after GBS, divided into PRHS and non-PRHS based on clinical assessment, and 14 control subjects (6 normal-weight, 8 with obesity) participated. All underwent a 3hour LMMTT and SMMTT during which glucometabolic responses as well as hypoglycaemic symptoms using the Edinburgh Hypoglycaemia Symptom Scale (EHSS) were assessed.
Results: During LMMTT, nadir glucose levels nor frequency of levels <70 mg/dl and <54 mg/dl did differ between the four groups. LMMTT could not differentiate between PRHS and non-PRHS in terms of total count of symptoms and the number of symptoms was not associated with low glycaemia. Remarkably, glycaemic values <54 mg/dl were only observed in the non-PRHS group. During SMMTT, glucometabolic responses were similar between PRHS and non-PRHS. There was no difference between PRHS and non-PRHS subjects in the incidence of glycaemia <70 mg/dl and the occurrence of glycaemia <54 mg/dl was extremely rare. Moreover, significantly low glycaemic levels <54 mg/dl were not found in healthy controls. Finally, significantly more hypoglycaemic symptoms were evocated in the PRHS group compared to non-PRHS during the second phase of SMMTT (from 75 to 120 minutes) with more neuroglycopenic and malaise symptoms in PRHS. Decrease rate of glucose was higher in PRHS subjects with malaise symptoms from 105-180 minutes compared to those without malaise.
Conclusion: Using a two-step approach of GCT and OGTT, up to 40% of OGTTs can be omitted, facilitating screening procedures for diabetes mellitus in people undergoing dialysis. This practical approach, should be further studied in order to help healthcare providers to identify and manage dysglycemia efficiently in this population.
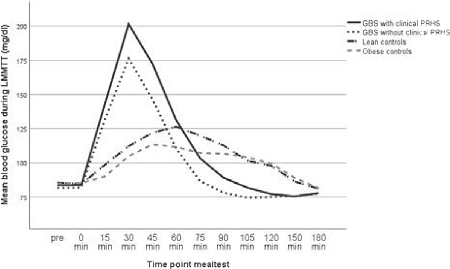
Figure 1. Mean glucose levels during LMMTT.
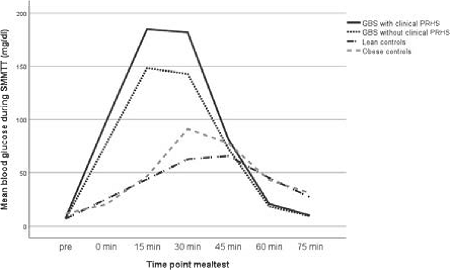
Figure 2. Mean glucose levels during SMTT.
}
Article tools
My recent searches
My recently viewed abstracts

Endocrine Abstracts
ISSN 1470-3947 (print) | ISSN 1479-6848 (online)
© Bioscientifica 2026 |
Privacy policy |
Cookie settings
BiosciAbstracts

Bioscientifica Abstracts is the gateway to a series of products that provide a permanent, citable record of abstracts for biomedical and life science conferences.
Find out more